Historically, healthcare has been reluctant to change. Prior to the COVID-19 pandemic, many healthcare organizations knew that a digital transformation was on the horizon, but they were dragging their feet to get there. Some would say COVID-19 put things in motion, others might argue COVID-19 catapulted telehealth into a standard of healthcare delivery.
In 2020 health systems launched new telehealth programs in response to the COVID-19 pandemic. One McKinsey survey revealed that the number of patients that had used telehealth increased from 11 percent in 2019 to 76 percent in 2020. Providers have seen 50 to 175 times the number of patients via telehealth than they did prior to the pandemic. Strategies that often take months, or even years, were put together in weeks, as telehealth programs were launched across the country. The day-to-day of healthcare providers (and patients) was turned on its head - everyone was forced to rethink how healthcare would be delivered and received safely.
Michigan Medicine and Emerest Health Rise to the Occasion
During the Vision to Virtual conference, Michigan Medicine and Emerest Health presented on how their respective organizations launched a Telehealth and RPM program in response to the COVID-19 pandemic.
The session began with Brandy Knudson, Virtual Care Project Manager and Dr. Grace Jenq, Associate Clinical Professor, Geriatric and Palliative Medicine, both of Michigan Medicine, discussing their decision to begin a telehealth program. For Michigan, the desire to start a remote monitoring program goes back, back to 2018 actually. They already knew “post acute remote patient monitoring provides the greatest benefit to patients and health systems due to providing greater continuity of care.” The COVID-19 pandemic set everything in motion.
During their session, Knudson and Dr. Jenq discussed the goal of their Patient Monitoring at Home (PMAH) program: “to increase capacity across the health system, be innovative in the post-acute space, and avoid unnecessary hospital and ED visits.” To achieve these goals, Michigan Medicine offers telehealth and RPM to engage with patients and families during the 30 day post hospitalization period - the time when patients are especially vulnerable.

Avoiding the “Voltage Drop” When Patients Return Home
On the topic of post hospitalization, Dr. Jenq elaborated: “it’s actually quite surprising that we haven't had more monitoring in this vital period. Patients will go from being in the hospital where they’re getting vital signs every 8 hours, they’ve got lots of support….and we send them home. And when we send them home there’s this voltage drop. There’s no one to check in, there’s no vitals taken, there’s no one to see how the patient is doing.”
Through the PMAH program, Michigan Medicine continues the care for patients in the post hospitalization period. They make sure that there is no voltage drop - patients are given tools for patient engagement and intervened with proactively, ensuring unnecessary 30 day readmission and ED visits are reduced.
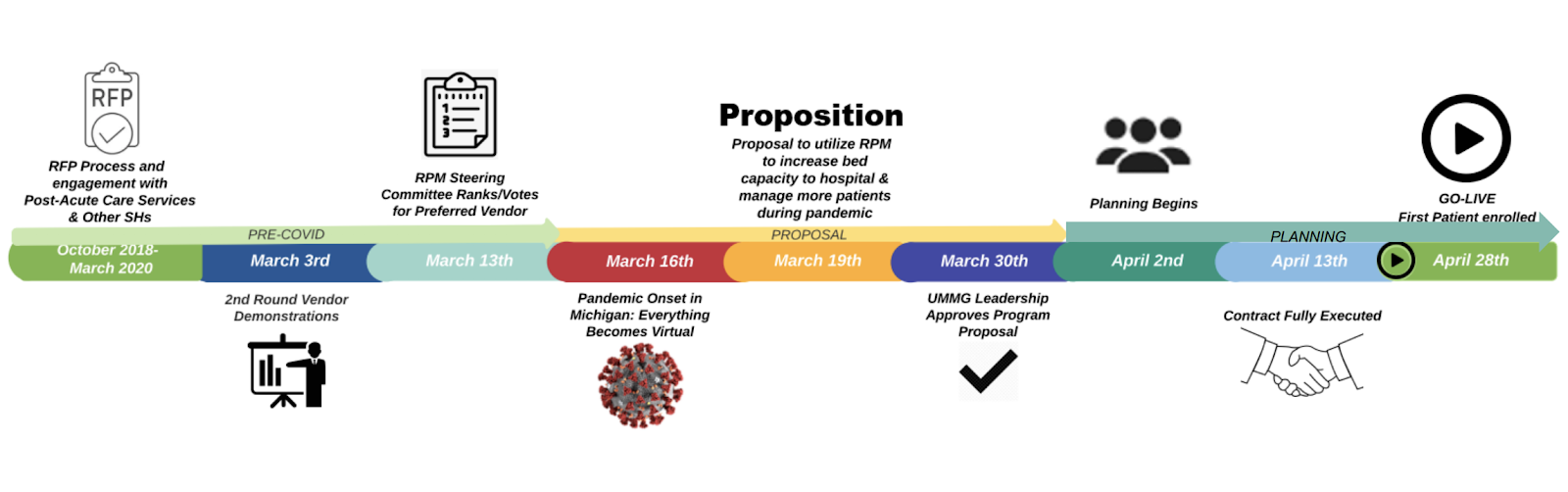
Michigan Medicine’s Implementation Timeline
Increasing Capacity, Improving Continuity of Care
Michigan Medicine includes as many patients as possible in their PMAH program - both COVID-19 patients, but also patients with chronic conditions who would benefit from telehealth at home. “We’re targeting high risk patients coming out of the hospital or skilled nursing facility and we’re being pretty broad. We’re actually saying ‘if you think this patient is high risk or has a readmission risk stratification of moderate to high we’re asking for folks to put in a referral. We also have a respiratory clinic where we see COVID patients...from the respiratory clinic if we have a person under investigation, or they have a diagnosis of COVID, we can help them with [remote monitoring at home],” said Dr. Jenq on the topic of inclusion criteria.
The PMAH program has been especially helpful with surge capacity during the pandemic. As more and more patients were going to the hospital with COVID-19 symptoms, Michigan Medicine had to figure out a way to free up beds - PMAH was a huge part of the solution.
.png?width=3330&name=Grace%20Jenq%20Quote%20(1).png)
Emerest Health Throws Out The Old Playbook
Prior to COVID-19, Emerest Health was fully aware of the benefits and the value of telehealth. They were using it in various ways across all 5 boroughs of New York City, their multiple east coast and midwest locations and across many different patient populations. While Emerest was already leveraging telehealth, the pandemic completely shifted how they operated and how they used the technology - “this situation, working within a global pandemic, presented its own set of unique challenges and really required throwing out the old playbook and anything we had used in the past and coming up with a new playbook, a new set of guidelines, a new set of protocols, a new set of policies on how we could really advance this program for the betterment and the health and safety of our patients.” stated Ethan Heimowitz, Administrator at Emerest at the top of his presentation.
Telehealth Technology Makes the Difference
From the onset of the pandemic, Emerest identified telehealth as how they would really be able to assist their patients - “when the pandemic started in March nobody knew what to expect. NYC was getting hit the hardest. Specifically in the Bronx, where many of our patients are serviced, they are living in areas where they might not have access to the best healthcare, it’s challenging at the best of times to adequately assess and assist them in their care. We believed that in order for them to stay healthy and safe during this pandemic, we needed to find a better way to assist them... we honed in on remote patient monitoring.”
Emerest serves the most at risk patient populations in New York City - the elderly, the poor, the patients that are in the most at-risk areas. At the onset of the pandemic, NYC, as the epicenter of the disease, was the most at risk area in the country. All populations in NYC were vulnerable to infection - “people were scared, aides were not going into patients’ homes, people did not want to ride public transportation, they were not interested, they just wanted to stay home and hopefully ride this out for the best” mentioned Heimowitz.
Full Scale Deployment Across 5 NYC Boroughs
Emerest deployed 700+ telehealth kits in just over a month across the 5 boroughs of NYC. It was full steam ahead in getting telehealth into patients’ homes. At first, patients responded with apprehension, telehealth was brand new to many patients - “it took encouragement and support to explain to them that this is something that’s meant to protect them at home if they don’t want to go to the hospital,” stated Heimowitz on the topic of patient buy-in.
The challenges Emerest faced during their roll-out were cumbersome. Ranging from patient buy-in to coordination, PPE shortages, changing city and stage guidelines, fears of patients and staff, working across all 5 NYC boroughs, their challenges really ran the gamut.
But they holstered their resources and emphasized the importance of getting telehealth into patients’ homes - equipping patients with the tools they needed to manage their health at home was, and remains, the priority.
Expanding Settings of Care with Telehealth & RPM
The resounding theme across both presentations was the importance of meeting patients where they are - at home. “As a health industry we really need to be thinking about how we can provide other settings in which we can care for people” mentioned Dr. Jenq during her presentation. Telehealth and RPM are doing just that by bringing care into the home.
Heimowitz closed out his session with a resounding endorsement of telehealth as a beneficial service for patients, “the 24/7 virtual care was really a game changer for these patients. When an aide went home at the end of the day, patients thought that was the beginning and end of their care. Now that they have this device, this was really a way for them to increase their exposure to healthcare, to realize that healthcare did not have to end when the aide left the home. They really have real-time live access to healthcare professionals that can assist them.”